‘How can we help?’ New roles and challenges for cardiothoracic trainees during COVID-19

29 Sep 2020
David Bleetman and Jacob Chacko
David Bleetman and Jacob Chacko are cardiothoracic trainees (NTN) in the London deanery based at King’s College Hospital. In this blog series, they detail their responsibilities in the intensive care unit, describe the requirements needed to maintain an on-call service, and as a second wave approaches, they highlight their eagerness to help again.
Like many non-critical care doctors, the cardiothoracic team at King’s College Hospital (KCH) saw significant disruption to normal working practices. Finding roles and ways in which we could help was challenging, but we soon found ourselves working as part of a diverse cadre that supported our colleagues in critical care.
Impact on normal activity
The South London boroughs of Southwark and Lambeth have a combined population of 700,000, and by April 2020, had recorded more than 800 COVID-19 cases each. The first cases of COVID-19 at KCH were confirmed on 4 March and rose steadily to 41 cases by 13 March. Nationally, there had been 798 positive cases and 10 confirmed deaths by the same date. At this stage, a number of changes to our clinical practice were made including cancelling all elective operations and converting outpatient appointments to telephone consultations. Shortly after, we were told that our elective ward was to be converted into a COVID-19 negative general intensive care unit (ICU), to make space for COVID-19 positive patients in existing ICU units (Figures 1 and 2).
By 30 March, there were 417 COVID-19 positive cases at KCH, with 31 confirmed COVID-related deaths. To accommodate the increasing numbers of admissions, patients who had been transferred to the cardiothoracic elective ward were stepped-down where possible or transferred to the few remaining COVID-19 negative critical care beds. COVID-19 positive cases were then transferred into our ward and cardiothoracic trainees were now directly involved in their care. Throughout, a 24-hour on-call service was provided for remaining inpatients and trauma cases.
Figure 1: Changing environment – a patient bay in our elective cardiothoracic ward converted into storage space for ICU equipment

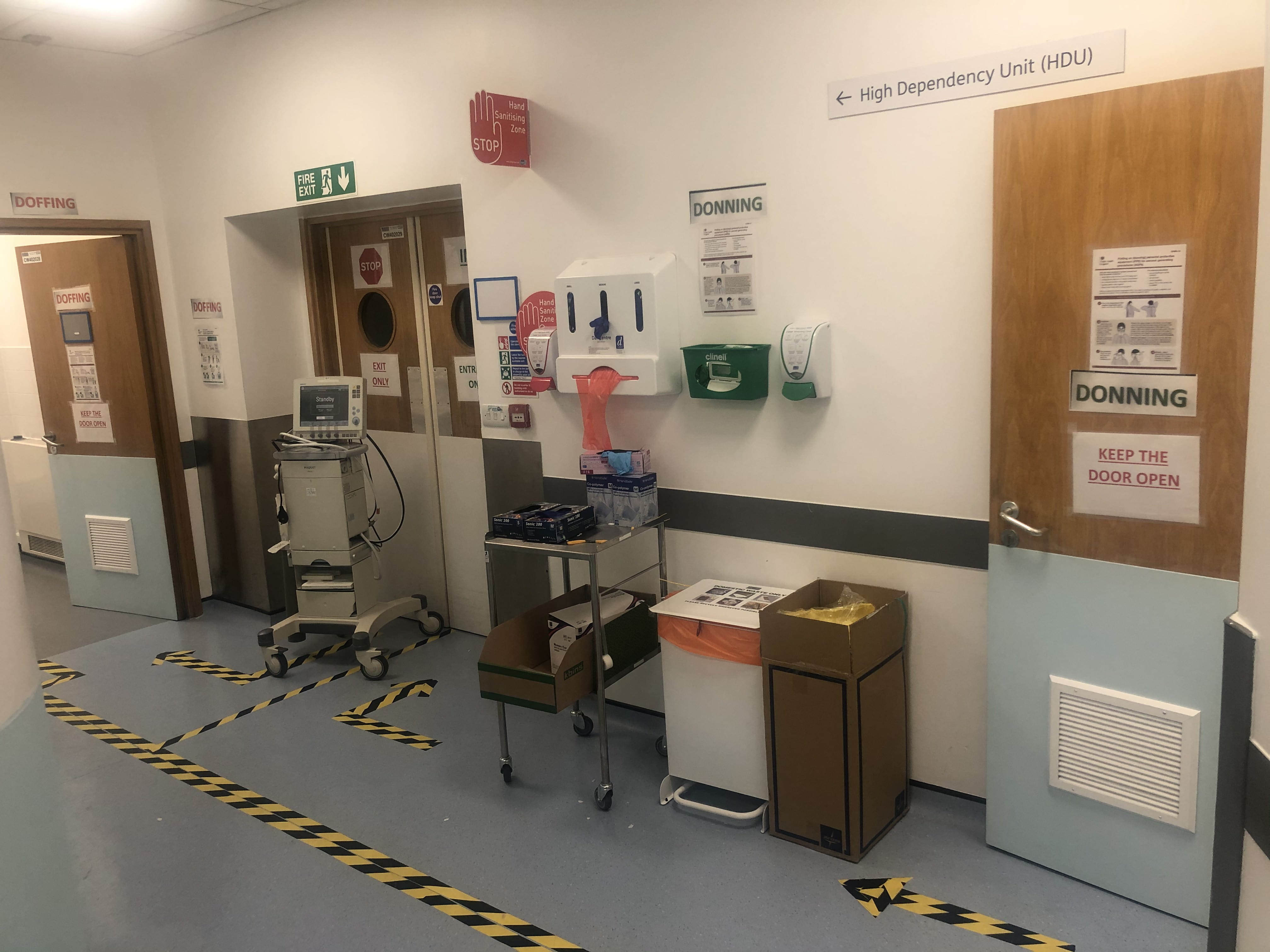
Figure 2: Entrance to our cardiothoracic high dependency unit, now COVID-19 positive ICU, with areas for donning and doffing personal protective equipment
Role in COVID-19 positive critical care units
By mid-March, it became clear that we would likely be asked to work in unfamiliar roles. The first sign of this was an email circular asking for our ICU experience, home distance from the hospital and any health problems that may put us at risk. An induction session for the ICU was held with lectures covering the basics of ICU care as well as COVID-specific teaching.
Despite the primers on ventilator settings and the disease process of the virus, the primary role of our surgeons in these new ICU teams was largely (at least initially) supportive. Our junior surgeons went from leading ward rounds, making treatment decisions and performing complex procedures, to documenting during ward rounds, filling in drug charts, and helping nurses change patients’ sheets; anything to ease the burden on our other team members and help treat or keep our patients comfortable. Later, some of us spent entire 12-hour shifts as part of a ‘proning team’, helping manoeuvre patients safely into a face-down position to help utilise healthy portions of their lungs.
Personal protective equipment and anxiety
Seeing our activity, roles and wards change dramatically over the space of a short few weeks was understandably disorientating for our doctors. This was compounded by ever-changing advice on personal protective equipment (PPE), equipment requirements and concerns over availability (there was a shortage of eye protection throughout, meaning visors needed to be thoroughly disinfected and re-used).
In our cardiothoracic department, due to the rapid deterioration many of these patients exhibit and the limited number of interventions available to stabilise and improve them, both medical and nursing staff who were accustomed to managing routine cardiothoracic surgery patients have found this period in their professional careers highly challenging. The nursing staff in particular were now at the very frontline and would closely observe the rapid deterioration and often death of a large number of patients. Given the speed and intensity of the COVID-19 pandemic, staff from all non-critical care specialties have had to face this reality with minimal preparation and training.
Our trust and local community responded. A ‘wellbeing zone’ was established by KCH for staff to spend time away from the wards and recuperate. This provided an opportunity to talk to colleagues as well as representatives from faith or spiritual groups. Local businesses were enthusiastic about donating food and products from businesses that had not long shut their doors. It is hard to describe the tremendous amount this did to validate the work done by all staff.
On-call challenges
Outside of the ICU, our trainees were still required to provide an on-call service for cardiothoracic emergencies. One of the unexpected consequences of the COVID-19 pandemic has been a steady referral for interventions requiring specialist input either relating to the disease process, or complications of necessary treatment. Informal discussions with other non-critical care colleagues have confirmed that this is a phenomenon not limited to cardiothoracic surgery.
An increase in referrals for ventilated patients with small pneumothoraces (air escaping into the chest cavity from damaged lungs, causing lung collapse) was seen. These referrals represented a difficult decision for the on-call registrar, as in normal circumstances the risk of injuring the lung further outweighs the potential benefit of relieving a small pneumothorax. In addition, there was a risk of deterioration associated with disconnecting the patient from mechanical ventilation for insertion of a drain, and the risk of exposure to all members in the vicinity of drain insertion. However, we recognise that many of these referrals were for young patients who were rapidly deteriorating, with a pneumothorax (however small) the only potentially reversible contributing factor.
The ensuing discussions with our critical care colleagues were difficult. Fortunately, the situation was mitigated by the early involvement by consultants in our department, producing and circulating clear guidance on the indications for drain insertion and initiating a consultant-to-consultant discussion to resolve any disagreement.
Conclusion
We have recently seen a concerning rise in the number of cases of COVID-19, and our Chief Medical Officer has warned of cases approaching 50,000 a day in a short number of weeks. It is therefore inevitable that our experiences will soon be called upon again. One question which we didn’t know how to answer fully in March was, how can we help? We now know. In the ICU, we can: make the ward round proceed smoothly, help our nursing colleagues change and turn patients or take an anaesthetic colleague through a tracheostomy. In our on-call roles: having the empathy and flexibility to appreciate that our colleagues are often searching for a reversible part of a disease process that can turn the outlook for a patient around, but being strong in our resolve to first ‘do no harm’ if an intervention will do just that. And in the break rooms: being a sensitive ear as well as a first-hand source of confidence that most of our COVID-19 patients do get better and that our colleagues work in these difficult times is appreciated.
This blog is from our series COVID-19: views from the NHS frontline. If you would like to write a blog for us, please contact content@rcseng.ac.uk.